
[box type=”bio”] What to Learn from this Article?[/box]
Diagnosis of sleeve fracture requires understanding epidemiology, and surgical operation is useful for its treatment.
Case Report | Volume 6 | Issue 5 | JOCR November-December 2016 | Page 24-27 | Masanori Tsubosaka, Takeshi Makino, Shin-ichiro Kishimoto, Kohei Yamaura. DOI: 10.13107/jocr.2250-0685.614
Authors: Masanori Tsubosaka[1], Takeshi Makino[1], Shin-ichiro Kishimoto[1], Kohei Yamaura[1]
[1] Department of Orthopaedic Surgery, Rokko Island Konan Hospital, 2-11, Koyo-Cho Naka, Higashinada-Ku, Kobe, 658-0032, Japan.
Address of Correspondence
Dr. Takeshi Makino,
Department of Orthopaedic Surgery, Rokko Island Konan Hospital, 2-11, Koyo-Cho Naka, Higashinada-Ku, Kobe, 658-0032, Japan.
Phone: 81-78-858-1111, Fax: 81-78-858-1110.
E-mail: macky@bf7.so-net.ne.jp
Abstract
Introduction: Sleeve fractures of the patella are rare fractures that only occur in children. The diagnosis is difficult both clinically and radiologically since the distal bony fragment may be too small to be detectable by radiography. A high-riding patella and hemarthrosis are important signs of sleeve fractures.
Case Presentation: A 12-year-old boy was admitted to the emergency room after having felt a severe pain in his left knee on kicking the ground while skateboarding earlier that day. Knee swelling, tense hemarthrosis, and periarticular tenderness were noted. On physical examination, an extension lag of 15 was observed. The active range of motion of the injured knee was 45-90° of flexion. Radiography showed an avulsion fracture of the lower pole of the patella and a high-riding patella. At the next day after the injury, we performed open reduction and internal fixation surgery. Open reduction with transosseous tunneling and cerclage wiring was performed because the distal bony fragment was too small for tension band wiring to be used. At 9 months after surgery, there was no extension lag, and the active range of motion of the injured knee was 0-140° of flexion. Callus formation over the fracture site and bone union was confirmed, and the cerclage wire was removed. To date, he had no further symptoms and has been able to carry out all types of physical activities, including skateboarding.
Conclusion: Although sleeve fractures in children are uncommon, it should be considered a possibility in children with a chief complaint of pain around the knee. Open reduction and internal fixation was effective in the treatment of sleeve fracture of the patella.
Keywords: Sleeve fracture, open reduction, internal fixation.
Introduction
Fractures of the patella are common injuries in adults but a relatively rare occurrence in children [1, 2]. The patella is a sesamoid bone and considered part of the quadriceps extensor mechanism. The incidence of patellar fractures in skeletally immature patients is low, however, among skeletally immature children, sleeve fractures of the patella are the most common type of patellar fractures. Sleeve fractures are caused by rapid muscle construction, and mostly affect children between 8 and 12 years of age [3]. This fracture often involves the lower pole of the patella in the form of an osteochondral avulsion. It can be easily missed on plain radiographs since only a small fragment of bone may be seen. In many cases, a high-riding patella on a plain radiograph may be the only and most prominent sign. In severely displaced sleeve fractures, open reduction and internal fixation are needed to achieve good clinical results [4, 5]. Conservative management may result in weakness of the extensor mechanism due to the high-riding patella and ossification of the patellar tendon. We present a case of sleeve fracture of the patella in a child and discuss the diagnostic modalities and treatment options for such fractures.
Case Report
A 12-year-old boy was admitted to the emergency room after having felt a severe pain in his left knee on kicking the ground while skateboarding earlier that day. Knee swelling, tense hemarthrosis, and periarticular tenderness were noted. On physical examination, an extension lag of 15° was observed. The active range of motion of the injured knee was 45-90° of flexion. Radiography showed an avulsion fracture of the lower pole of the patella and a high-riding patella (Fig. 1). The injured knee had an Insall-Salvati ratio of 1.48. Sleeve fracture of the patella was diagnosed clinically based on the signs of a high-riding patella and a gap in the extensor mechanism at the lower pole of the patella. At the next day after the injury, we performed open reduction and internal fixation surgery.
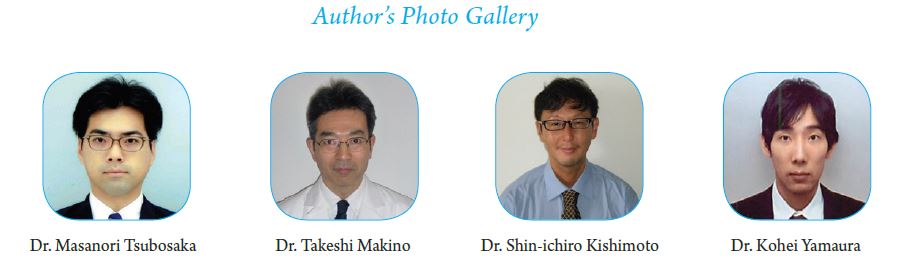
During surgery, we found that half of the articular cartilage of the patella and a corresponding portion of the patellar retinaculum were avulsed, together with a small fragment of bone (Fig. 2).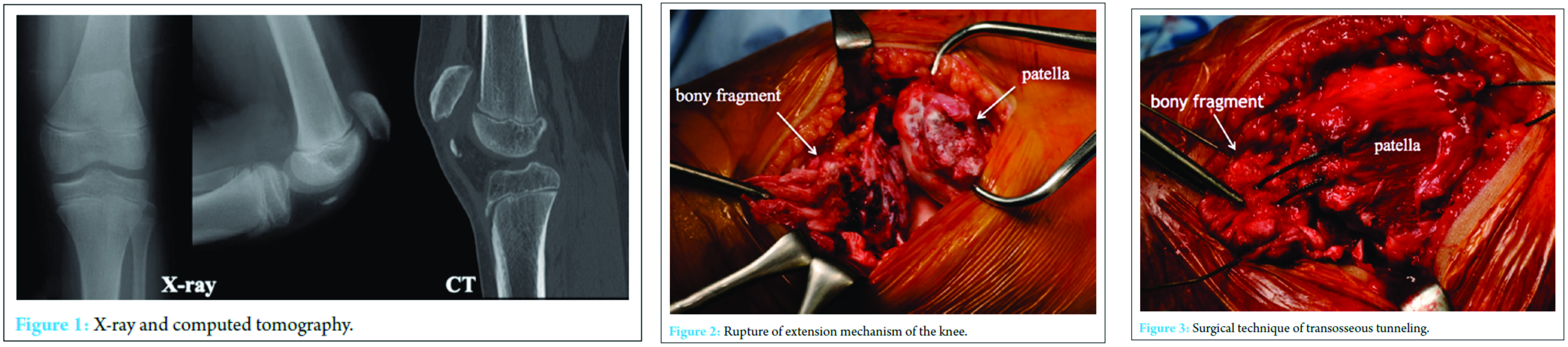 Initially, we tried to perform open reduction with tension band wiring, but the distal bony fragment was too small to be laced by Kirschner wire. We subsequently sutured the patella tendon from the distal to proximal portion with polyester suture thread (No. 5 ETHIBOND®), similarly to a Bunnell method, and inserted a needle into two sites of the distal bony fragment. We made two bone tunnels in the direction of the long axis on the proximal bony fragment, and can each thread through these bone tunnels (Fig. 3). We confirmed the distal bony fragment to be reduced and in a good position, and performed knot-tying on the upper pole of the patella. Subsequently, we performed cerclage wiring of the patella tendon, soft tissue around the patella, and quadriceps tendon using laced soft wire. Finally, we sutured the patellar retinaculum as reinforcement. The immediate post-operative Insall-Salvati ratio was 0.92 (Fig. 4).
Initially, we tried to perform open reduction with tension band wiring, but the distal bony fragment was too small to be laced by Kirschner wire. We subsequently sutured the patella tendon from the distal to proximal portion with polyester suture thread (No. 5 ETHIBOND®), similarly to a Bunnell method, and inserted a needle into two sites of the distal bony fragment. We made two bone tunnels in the direction of the long axis on the proximal bony fragment, and can each thread through these bone tunnels (Fig. 3). We confirmed the distal bony fragment to be reduced and in a good position, and performed knot-tying on the upper pole of the patella. Subsequently, we performed cerclage wiring of the patella tendon, soft tissue around the patella, and quadriceps tendon using laced soft wire. Finally, we sutured the patellar retinaculum as reinforcement. The immediate post-operative Insall-Salvati ratio was 0.92 (Fig. 4).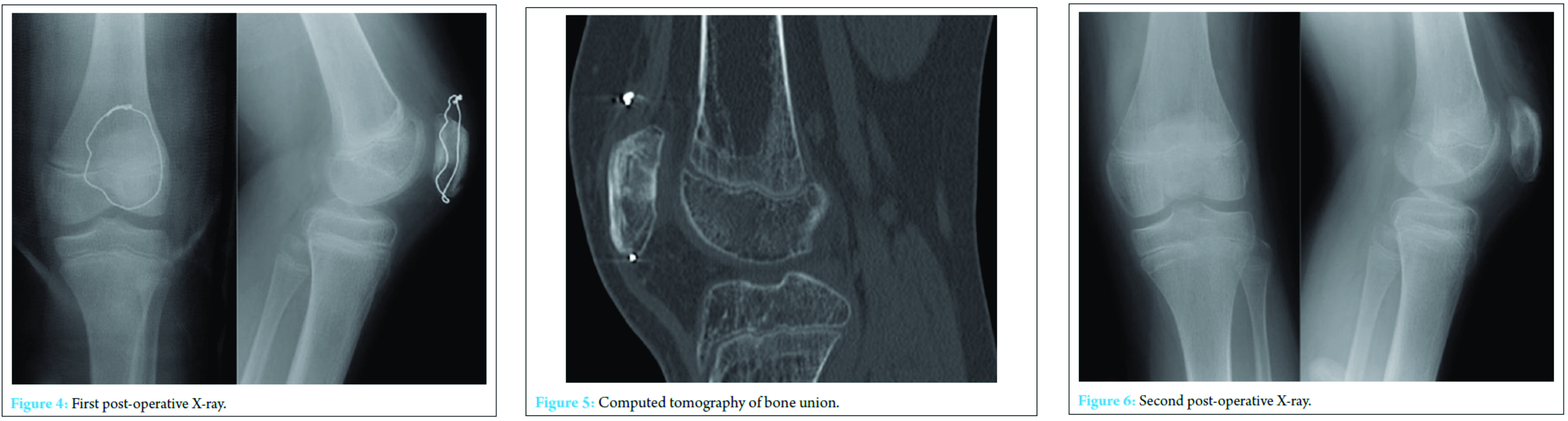
The knee joint was immobilized in a cylinder cast for 4 weeks after surgery. Physical rehabilitation was started, and eventually, the patient made a successful recovery. At 9 months after surgery, there was no extension lag, and the active range of motion of the injured knee was 0-140° of flexion. Callus formation over the fracture site and bone union was confirmed (Fig. 5), and the cerclage wire was removed (Fig. 6). To date, he had no further symptoms and has been able to carry out all types of physical activities, including skateboarding. The patient and his parents were asked if data concerning the case could be submitted for publication, and they consented.
Discussion
We presented a case of sleeve fracture of the patella in a child and described its successful treatment with open reduction with transosseous tunneling and cerclage wiring.
The incidence of patella fractures in children is much lower than that in adults, which may be due to either a lower number of children sustaining knee injuries or due to special anatomic characteristics of the knee in children. Children have softer and more flexible ligaments, as well as articular capsule and cartilage, and thus, more joint laxity is provided to keep the patella from injury. Furthermore, the patella is mainly composed of cartilage, allowing the bony component of the patella to avoid fracture [6].
The mechanism of sleeve fracture is a rapid contraction of the quadriceps on a flexed knee. Sleeve fractures usually occur in individuals involved in explosive acceleration activities such as jumping, although high-energy sports such as skateboarding are now also considered common causes [5].
Because the distal bony fragment in sleeve fractures is often very small, the correct diagnosis may be delayed or missed altogether. Thus, we think that it is important to listen carefully the clinical history, which generally involves a sudden onset of severe pain after an explosive acceleration such as jumping rather than a fall, and the symptoms, which include pain and a swollen knee. Moreover, we think two clinical signs were very important: First, a palpable gap at the lower pole of the patella, and second, a high-riding patella. If there is no gap or high-riding patella, magnetic resonance imaging can be useful to identify avulsion of the lower pole of the patella [7, 8], and the diagnosis can be confirmed by ultrasound [9]. Although diagnosis may be difficult in the presence of pain and tense hemarthrosis, an awareness of the injury together with the characteristic radiological features should confirm the diagnosis.
The treatment for sleeve fractures of the patella is anatomical reduction and reconstruction of the extensor mechanism. If a bony fragment is visible on radiography and the displacement is <2 mm, conservative treatment with cast immobilization in the extended position of the knee joint is indicated. However, the results of conservative treatment are often unsatisfactory [5, 10]. If surgery is performed properly without delay, the good results have been reported, except the slight limitation of the knee flexion [6, 11]. The surgical repair method is generally selected dependent on the surgeons’ personal preference. Large transosseous sutures are simple and efficient [12, 13], and a modified tension band wire system or even intraosseous anchors can moreover be used [14]. Here, we performed open reduction and internal fixation with a polyester suture thread and cerclage wiring by soft wire; these procedures were shown to be effective in our case.
Conclusion
Although sleeve fractures of the patella in children are uncommon, we should think one of the differential diagnoses, in cases of acute knee injuries, especially when the injury was caused by an explosive force such as jumping. Because the diagnosis can be often missed, especially in fractures with a very small avulsed bony fragment. We suggest that early surgical intervention achieved a satisfactory result for the displaced sleeve fractures of the patella.
Clinical Message
Diagnosing sleeve fracture is difficult both clinically and radiologically since the distal bony fragment may be too small to be detectable by radiography. Open reduction with transosseous tunneling and cerclage wiring can become a useful procedure if the distal bony fragment is too small for tension band wiring to be used.
References
1. Boström A. Fracture of the patella. A study of 422 patellar fractures. Acta Orthop Scand Suppl 1972;143:1-80.
2. Crawford AH. Fractures about the knee in children. Orthop Clin North Am 1976;7(3):639-656.
3. Hunt DM, Somashekar N. A review of sleeve fractures of the patella in children. Knee 2005;12(1):3-7.
4. Ray JM, Hendrix J. Incidence, mechanism of injury, and treatment of fractures of the patella in children. J Trauma 1992;32(4):464-467.
5. Houghton GR, Ackroyd CE. Sleeve fractures of the patella in children: a report of three cases. J Bone Joint Surg Br 1979;61(2):165-168.
6. Dai LY, Zhang WM. Fractures of the patella in children. Knee Surg Sports Traumatol Arthrosc 1999;7(4):243-245.
7. Bates DG, Hresko MT, Jaramillo D. Patellar sleeve fracture: demonstration with MR imaging. Radiology 1994;193(3):825-827.
8. Shands PA, McQueen DA. Demonstration of avulsion fracture of the inferior pole of the patella by magnetic resonance imaging. A case report. J Bone Joint Surg Am 1995;77(11):1721-1723.
9. Lin SY, Lin WC, Wang JW. Inferior sleeve fracture of the patella. J Chin Med Assoc 2011;74(2):98-101.
10. Bruijn JD, Sanders RJ, Jansen BR. Ossification in the patellar tendon and patella alta following sports injuries in children. Complications of sleeve fractures after conservative treatment. Arch Orthop Trauma Surg 1993;112(3):157-158.
11. Gao GX, Mahadev A, Lee EH. Sleeve fracture of the patella in children. J Orthop Surg (Hong Kong) 2008;16(1):43-46.
12. Sponseller P, Stanitsk C. Fractures in Children. Philadelphia, PA: Lippincott, Williams and Wilkins; 2001. p. 1029.
13. Kaar TK, Murray P, Cashman WF. Transosseous suturing for sleeve fracture of the patella: case report. Ir J Med Sci 1993;162(4):148-149.
14. Ogata K. Painful bipartite patella. A new approach to operative treatment. J Bone Joint Surg Am 1994;76(4):573-578.
| How to Cite This Article: Tsubosaka M, Makino T, Kishimoto S, Yamaura K. A Case Report of Sleeve Fracture of the Patella in a Shield. Journal of Orthopaedic Case Reports 2016 Nov-Dec;6(5):24‑27. Available from: https://www.jocr.co.in/wp/2016/11/10/2250-0685-614-fulltext/ |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


