Metastatic adenoid cystic carcinoma to the dermis and subcutis of right breast
By Kulkarni M, Saxena R, Leonard DJ, Gupta P


CASE SUMMARY
A 65-year-old female presented to the breast care facility with a two-month history of a painful, palpable mass on the lateral aspect of her right breast, and a history of T3N0, stage III, adenoid cystic carcinoma (ACC) of the submandibular salivary gland with metastasis to the right lung. The patient stated the pain was episodic, sharp, and shooting with radiation along the lateral aspect of her right breast. She denied nipple discharge, nipple retraction, or skin dimpling. She had a previous history of atypical ductal and lobular hyperplasia and intraductal papilloma of the right breast. Physical examination showed a tender, 1 cm raised, superficial nodule located at the 9 o’clock axis of the right breast, along the anterior axillary line. There was no evidence of masses elsewhere in the breast, nipple retraction, nipple discharge, skin dimpling, or architectural distortion. Left breast abnormalities were not present.
IMAGING FINDINGS
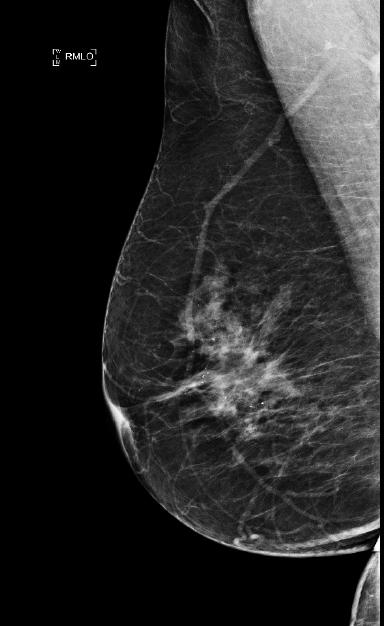
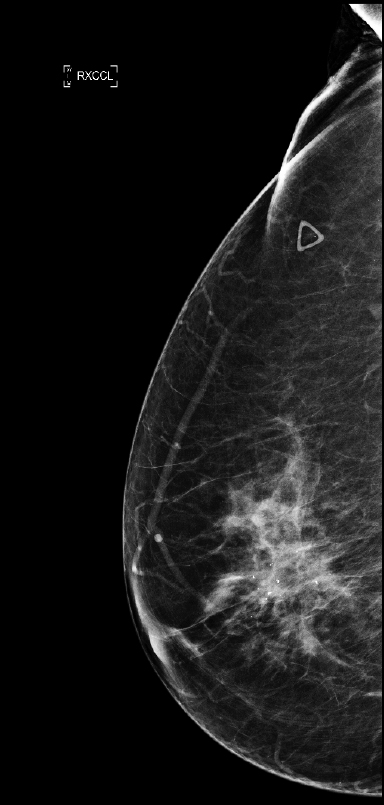
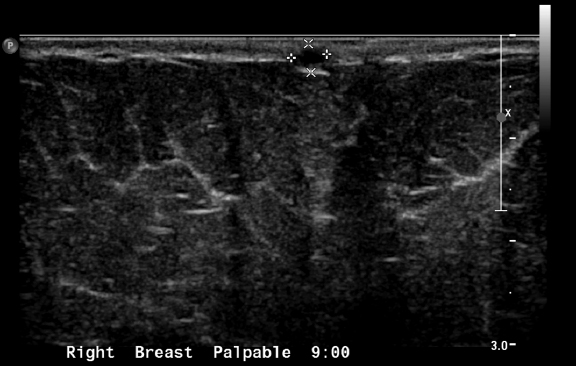
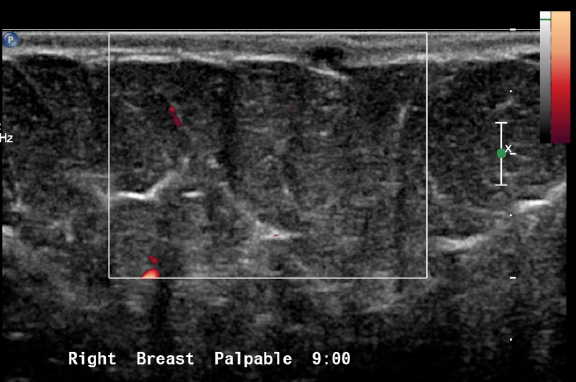
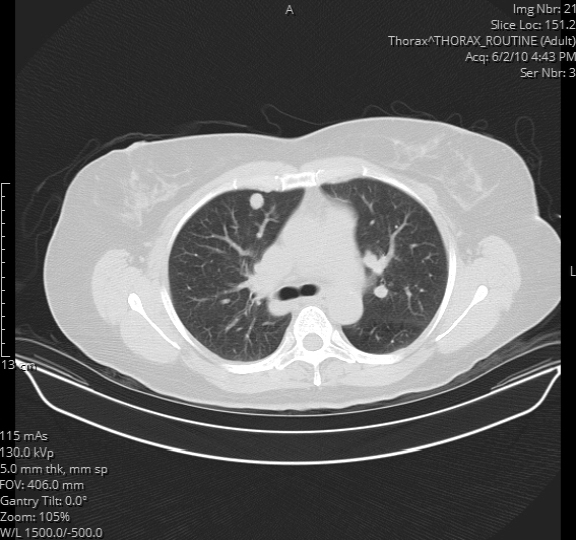
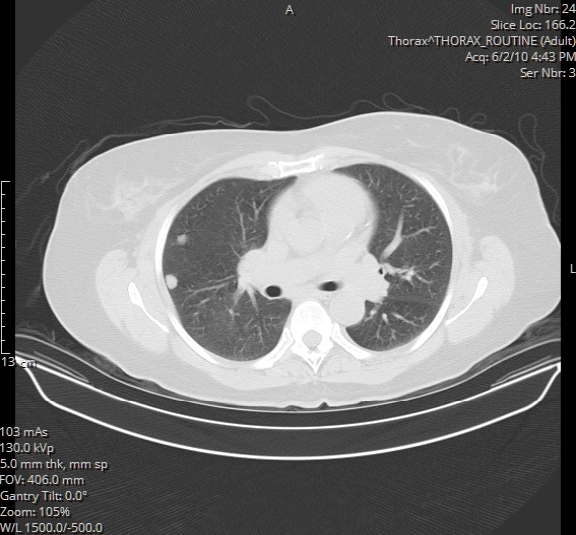
Initial workup for the palpable breast mass included bilateral diagnostic mammogram with tomosynthesis (Figures 1A and 1B) and right breast ultrasound (Figures 2A, 2B, 2C, 2D). The mammogram showed no abnormality in the region of the palpable lump. No suspicious mass or microcalcifications were seen. Expected postsurgical changes from a previous excisional biopsy for intraductal papilloma were seen. Targeted ultrasound of the palpable abnormality showed a 5 × 3 × 3 mm, hypoechoic, complicated cystic mass centered in the skin of the right breast, without abnormal vascularity. This was thought to represent a sebaceous cyst/epidermal inclusion cyst. The mass was therefore classified as Breast Imaging Reporting and Data System (BIRADS) 2: a benign finding. Also included out of interest are CT images of the chest performed 4 years prior (Figures 3A, 3B), showing lung metastases of salivary gland ACC. Despite these findings, a decision was made to surgically excise the palpable finding.
DIAGNOSIS
Metastatic adenoid cystic carcinoma to the dermis and subcutis of right breast
DISCUSSION
Adenoid cystic carcinoma is the second most common malignancy of the salivary glands1. However, cutaneous metastasis of this malignancy is rare.1 Cutaneous metastases from malignancies of the salivary gland account for 2% of all cutaneous metastases in men and 1% in women.1 The anterior chest wall and abdomen are the most common sites for cutaneous metastasis in women2. Of the malignancies that metastasize to the skin, carcinomas are the most common, but sarcomas, lymphomas and leukemias contribute to a large percent of skin metastases as well3.
Our patient presented initially with a palpable, right breast/lateral chest wall mass. The usual protocol of imaging with diagnostic mammography and sonography was followed. On such imaging, masses seen within the layers of the skin are considered benign, and the differential diagnoses for such masses include sebaceous cysts and epidermal inclusion cysts. It is difficult to differentiate between epidermal inclusion cysts and sebaceous cysts on the basis of their appearance on imaging studies.4 At mammography, these cysts may be seen as masses with circumscribed margins with variable tissue density.4 On ultrasound, they can range from cystic to more solid in appearance, depending on their contents.4 They are circumscribed or may be irregular when they are inflamed. Percutaneous biopsy of a sebaceous cyst/epidermal inclusion cyst is relatively contraindicated due to the risk of extensive local inflammation caused by dissipated contents of the cyst. Such findings on imaging are classified as benign using the BIRADS classification. The recommendation is to continue routine screening.5
This patient had a past medical history of ACC of the salivary gland diagnosed nine years ago. She underwent excision of a left submandibular gland along with a left selective neck dissection, followed by radiation therapy. She did well for the next four years until a surveillance CT scan of the chest found multiple pulmonary nodules. The nodules were confirmed as metastatic ACC, for which she underwent right upper lobectomy and middle lobe resection. She was then asymptomatic for the next four years, until she presented at this visit.
Our patient underwent elective excision of the breast skin mass, as it was very painful. Pathologic examination of the mass revealed metastatic ACC of the dermis and subcutaneous tissue. The tumor was morphologically identical to the previous metastasis to the lung. It was present in several foci, some of which may have been intravascular. Some foci were adjacent to the superior and deep margins. Immunostains for tumor prognostic markers were performed as requested by the oncologist, revealing estrogen receptor positive (1% of cells), progesterone receptor positive (10% of cells) and Her2-neu negative.
CONCLUSION
Though rare, metastatic deposit in the skin should be part of the differential diagnosis for a benign-appearing mass of the skin. A high index of suspicion must be maintained for patients with a history of malignancy presenting with a new breast mass that may appear benign on imaging.
REFERENCES
- Yurut-Caloglu V, Caloglu M, Ozyilmaz F, et al. Lung, bone, skeletal muscles and cutaneous metastases from adenoid cystic carcinoma of the parotid gland: A case report and review of the literature. Medical Oncol. 2007;24(4):458-62.
- Hussein MR. Skin metastasis: A pathologist’s perspective [Abstract]. J Cutan Pathol. 2010;Sep;37(9).
- Nibhoria S, Tiwana KK, Kaur M, et al. A Clinicopathological and Immunohistochemical Correlation in Cutaneous Metastases from Internal Malignancies: A Five-Year Study. J Skin Cancer. Epub 2014 Aug 25.
- Giess C, Raza S, Birdwell R. Distinguishing Breast Skin Lesions from Superficial Breast Parenchymal Lesions: Diagnostic Criteria, Imaging Characteristics, and Pitfalls. Radiographics. 2011: Nov-Dec;31(7):1959-72.
- Eberl M, Fox C, Edge S, et al. (2006). BI-RADS Classification for Management of Abnormal Mammograms. J Am Board Fam Med. 2006: Mar-Apr;19(2):161-4.