
Abstract
Background
Enhanced recovery after surgery (ERAS) colorectal guideline implementation has occurred primarily in standalone institutions worldwide. We implemented the guideline in a single provincial healthcare system, and our study examined the effect of the guideline on patient outcomes [length of stay (LOS), complications, and 30-day post-discharge readmissions] across a healthcare system.
Methods
We compared pre- and post-guideline implementation in consecutive elective colorectal patients, ≥18 years, from six Alberta hospitals between February 2013 and December 2014. Participants were followed up to 30 days post discharge. We used summary statistics, to assess the LOS and complications, and multivariate regression methods to assess readmissions and to estimate cost impacts.
Results
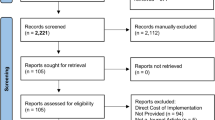
A total of 1333 patients (350 pre- and 983 post-ERAS) were analysed. Of this number, 55 % were males. Median overall guideline compliance was 39 % in pre- and 60 % in post-ERAS patients. Median LOS was 6 days for pre-ERAS compared to 4.5 days in post-ERAS patients with the longest implementation (p value <0.0001). Adjusted risk ratio (RR) was 1.71, 95 % CI 1.09–2.68 for 30-day readmission, comparing pre- to post-ERAS patients. The proportion of patients who developed at least one complication was significantly reduced, from pre- to post-ERAS, difference in proportions = 11.7 %, 95 % CI 2.5–21.0, p value: 0.0139. The net cost savings attributable to guideline implementation ranged between $2806 and $5898 USD per patient.
Conclusion
The findings in our study have shown that ERAS colorectal guideline implementation within a healthcare system resulted in patient outcome improvements, similar to those obtained in smaller standalone implementations. There was a significant beneficial impact of ERAS on scarce health system resources.




Similar content being viewed by others


References
Simpson JC, Moonesinghe SR, Grocott MPW et al (2015) Enhanced recovery from surgery in the UK: an audit of the enhanced recovery partnership programme 2009–2012. Br J Anaesth 115(4):560–568
Gustafsson UO, Scott MJ, Schwenk W et al (2013) Guidelines for perioperative care in elective colonic surgery: Enhanced Recovery After Surgery (ERAS®) Society recommendations. World J Surg 37:259–284. doi:10.1007/s00268-012-1772-0
Gustafsson UO, Scott MJ, Schwenk W et al (2012) Guidelines for perioperative care in elective colonic surgery: Enhanced Recovery After Surgery (ERAS®) Society recommendations. Clin Nutr 31:783–800
Nygren J, Thacker J, Carli F et al (2013) Guidelines for perioperative care in elective rectal/pelvic surgery: Enhanced Recovery After Surgery (ERAS®) Society recommendations. World J Surg 37:285–305. doi:10.1007/s00268-012-1787-6
Nygren J, Thacker J, Carli F et al (2012) Guidelines for perioperative care in elective rectal/pelvic surgery: enhanced recovery after surgery (ERAS®) Society recommendations. Clin Nutr 31:801–816
Walter CJ, Collin J, Dumville JC et al (2009) Enhanced recovery in colorectal resections: a systematic review and meta-analysis. Int J Colorectal Dis 11:344–353
Wind J, Polle SW, Jin PHPFK et al (2006) Systematic review of enhanced recovery programmes in colonic surgery. Br J Surg 93:800–809
Gouvas N, Tan E, Windsor A et al (2009) Fast-track vs standard care in colorectal surgery: a meta-analysis update. Int J Colorectal Dis 24:1119–1131
Adamina M, Kehlet H, Tomlinson GA et al (2011) Enhanced recovery pathways optimize health outcomes and resource utilization: a meta-analysis of randomized controlled trials in colorectal surgery. Surgery 149:830–840
Varadhan KK, Neal KR, Dejong CHC et al (2010) The enhanced recovery after surgery (ERAS) pathway for patients undergoing major elective open colorectal surgery: a meta-analysis of randomized controlled trials. Clin Nutr 29:434–440
Greco M, Capretti G, Beretta L et al (2014) Enhanced recovery program in colorectal surgery: a meta-analysis of randomized controlled trials. World J Surg 38:1531–1541. doi:10.1007/s00268-013-2416-8
Lv L, Y-f Shao, Y-b Zhou (2012) The enhanced recovery after surgery (ERAS) pathway for patients undergoing colorectal surgery: an update of meta-analysis of randomized controlled trials. Int J Colorectal Dis 27:1549–1554
Eskicioglu C, Forbes S, Aarts M-A et al (2009) Enhanced recovery after surgery (ERAS) programs for patients having colorectal surgery: a meta-analysis of randomized trials. J Gastrointest Surg 13:2321–2329
Roulin D, Donadini A, Gander S et al (2013) Cost-effectiveness of the implementation of an enhanced recovery protocol for colorectal surgery. Br J Surg 100:1108–1114
Lee L, Mata J, Ghitulescu GA et al (2014) Cost-effectiveness of enhanced recovery versus conventional perioperative management for colorectal surgery. Ann Surg 00:1–8
Gillissen F, Hoff C, Maessen JC et al (2013) Structured synchronous implementation of an enhanced recovery program in elective colonic surgery in 33 Hospitals in The Netherlands. World J Surg 37:1082–1093. doi:10.1007/s00268-013-1938-4
Bell GV (2008) Sample size. In: Statistical rules of thumb, vol 36, 2nd edn. John Wiley & Sons Inc., Hoboken, pp 1–14
Vittinghoff E, McCulloch CE (2007) Relaxing the rule of ten events per variable in logistic and Cox regression. Am J Epidemiol 165:710–718
Derksen S, Keselman HJ (1992) Backward, forward and stepwise automated subset selection algorithms: frequency of obtaining authentic and noise variables. Br J Math Stat Psychol 45:265–282
Vlug MS, Wind J, Hollmann MW et al (2011) Laparoscopy in combination with fast track multimodal management is the best perioperative strategy in patients undergoing colonic surgery: a randomized clinical trial (LAFA-study). Ann Surg 254:868–875
Delaney C, Zutshi M, Senagore A et al (2003) Prospective, randomized, controlled trial between a pathway of controlled rehabilitation with early ambulation and diet and traditional postoperative care after laparotomy and intestinal resection. Dis Colon Rectum 46:851–859
Gustafsson UO, Tiefenthal M, Thorell A et al (2012) Laparoscopic-assisted and open high anterior resection within an ERAS protocol. World J Surg 36:1154–1161. doi:10.1007/s00268-012-1519-y
Spanjersberg WR, Van Sambeeck JDP, Bremers A et al (2015) Systematic review and meta-analysis for laparoscopic versus open colon surgery with or without an ERAS programme. Surg Endosc 29(12):3443–3453
Group (2015) The impact of enhanced recovery protocol compliance on elective colorectal cancer resection: results from an international registry. Ann Surg 261:1153–1159
Van Bree S, Vlug M, Bemelman W et al (2011) Original research: faster recovery of gastrointestinal transit after laparoscopy and fast-track care in patients undergoing colonic surgery. Gastroenterology 141:872–880
Gustafsson UO, Hausel J, Thorell A et al (2011) Adherence to the enhanced recovery after surgery protocol and outcomes after colorectal cancer surgery. Arch Surg 146:571–577
Polle SW, Wind J, Fuhring JW et al (2007) Implementation of a fast-track perioperative care program: what are the difficulties? Dig Surg 24:441–449
Ahmed J, Khan S, Lim M et al (2012) Enhanced recovery after surgery protocols—compliance and variations in practice during routine colorectal surgery. Int J Colorectal Dis 14:1045–1051
Grant support
The ERAS project was funded by the Partnership for Research and Innovation in the Health System (PRIHS) research grant from Alberta Innovates: Health Solutions.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest
Dr. Ljungqvist is the current Chairman of the ERAS Society. He founded, serves on the Board and owns stock in Encare AB that runs the ERAS Society Interactive Audit System.
Additional information
Ljungqvist and Gramlich request shared senior authorship.
Rights and permissions
About this article

Cite this article
Nelson, G., Kiyang, L.N., Crumley, E.T. et al. Implementation of Enhanced Recovery After Surgery (ERAS) Across a Provincial Healthcare System: The ERAS Alberta Colorectal Surgery Experience. World J Surg 40, 1092–1103 (2016). https://doi.org/10.1007/s00268-016-3472-7
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00268-016-3472-7